| dc.contributor.author | Coulombe, A | fr_FR |
| dc.contributor.author | Deroubaix, E | fr_FR |
| dc.contributor.author | Coraboeuf, E | fr_FR |
| dc.date.accessioned | 2012-08-23T13:56:21Z | |
| dc.date.available | 2012-08-23T13:56:21Z | |
| dc.date.issued | 1999 | fr_FR |
| dc.identifier.citation | Coulombe, A - Deroubaix, E - Coraboeuf, E, Mécanismes ioniques des altérations de la repolarisation cardiaque dans les cardiopathies., Med Sci (Paris), 1999, Vol. 15, N° 3; p.359-68 | fr_FR |
| dc.identifier.issn | 1958-5381 | fr_FR |
| dc.identifier.uri | http://hdl.handle.net/10608/1346 | |
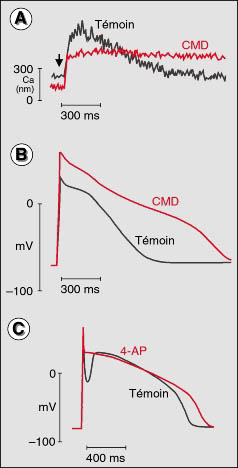
| dc.description.abstract | Parmi les alterations des courants ioniques cardiaques associes aux processus d' hypertrophie, de dilatation et de defaillance, la reduction du courant potassique transitoire sortant, Ito, s' avere la plus precoce et la plus constante. Ce courant, qui a pour effet de produire une encoche au debut du plateau des potentiels d' action longs, peut se reveler redoutable lorsque les courants entrants sont localement reduits par l' ischemie : il peut creuser l' encoche jusqu' a disparition soudaine de la plus grande partie du potentiel d' action, ce qui constitue une source majeure d' heterogeneite de repolarisation, productrice d' arythmies severes induites par re-entree. Dans ce cas, inhiber Ito serait benefique. Une augmentation du courant d' echange INa-Ca, par surcharge en calcium cytosolique et surexpression de l' echangeur, est associee a la defaillance et a la dilatation cardiaques et participe a l' allongement du potentiel d' action. Les alterations des autres courants ioniques (ICaL, IKI, Isus, INa-Ca) sont plus incertaines. | fr |
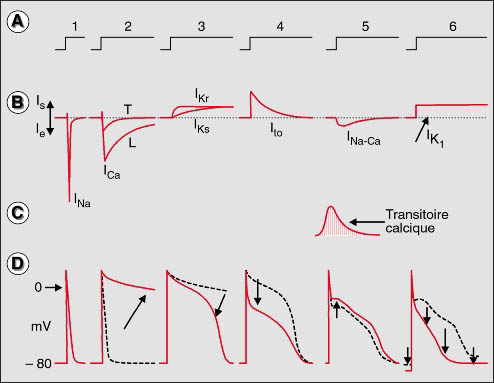
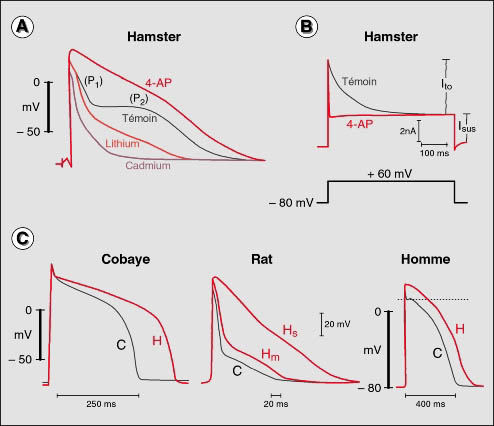
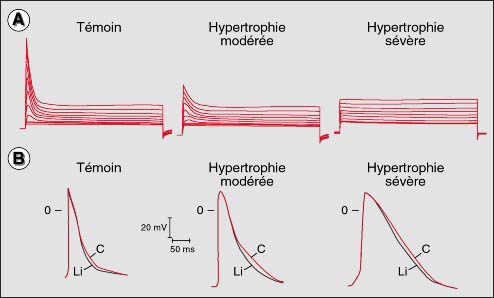
| dc.description.abstract | At the cellular level, each myocardial electrical event consists in a depolarization wave, the action potential, with a fast rising phase followed by a plateau of more or less complex shape depending on the species, the tissue and the recording area. The development of this depolarization wave results from inward ionic currents becoming larger than outward currents, whereas its decay, i.e. its repolarization, results from outward currents becoming larger than inward currents. In several pathological conditions (hypertrophy, dilation, heart failure, diabetes, etc.) the action potential is usually markedly lengthened, whereas the transient outward current, Ito known to induce a fast initial repolarization is reduced or suppressed. This is for example the case in moderate (partial reduction of Ito) and severe hypertrophy (almost complete suppression of Ito). Because Ito is a transient current it can control duration of brief action potentials as in human atrial myocytes but not that of long lasting action potentials as in human ventricular myocytes. In the latter it can induce mainly a very transient initial repolarization often forming a deep notch at the beginning of the plateau. In dogs and apparently also in humans Ito is almost absent in ventricular endocardial layers. In contrast, it is prominent in both epicardial and midlayers. When inward currents are depressed by ischemia, the notch can become locally so deep that a sudden loss of the major part of the plateau can occur, thus inducing a dramatic increase in repolarization heterogeneity, a situation known to be the source of severe ventricular arrhythmias. Because such an event requires a large Ito to occur, the Ito depression, or suppression, observed in several cardiopathies may be considered as a protective mechanism against certain ischemia-induced ventricular arrhythmias. Cardiac dilatation and failure are also frequently associated with action potential lengthening and Ito depression. Such alterations have been shown to occur in different animal models in which hypertrophy does not develop as shown by the absence of any increase in cell size and capacitance. The action potential lengthening observed in severe hypertrophy and dilation does not entirely result from Ito suppression. Other changes have been described in different models but not all, such as a decrease in the sustained outward current, Isus, or the background K current, IKl, and, more consistently, in increase in the sodium calcium exchange current, INa-Ca, whereas reported changes in calcium current ICaL, appear largely variable. ICaL remains frequently unchanged during hypertrophy whereas ICaL depression has been reported in some conditions of marked dilation. Cardiomyopathies are frequently associated with ventricular arrhythmias. They can result from re-entry, as in the case of an increased repolarization heterogeneity and/or fragmented conduction pathways. In the cardiomyopathic myocyte several sources of automatism can also result from currents which are poorly developed in the normal myocardium such as the low threshold calcium current, ICaT, or the pacemaker current, If, which can be more strongly activated in the diseased than in the normal heart. Recent developments in molecular biology have shown that repolarizing currents such as Ito and Isus result from activation of channels (alpha-subunits) of the Kv type which can belong todifferent subfamilies and can be composed of homo or heterotetramers from a given subfamily. The fact that Ito is a transient current whereas Isus is not, results from the presence in the Ito molecule of one or more (up to four) amino termini forming an inactivation gate of the "ball and chain" type which can occlude the activated channels. In addition beta subunits that are, or can be closely associated with Ito or Isus channels also possess an inactivation gate that can inactivate non-inactivating channels or accelerate inactivation of inactivating channels, thus complicating the analysis of Ito. Notwithstanding this complexity, a successful correction of action potential lengthening in cells from failing heart by adenoviral gene transfer has been reported. | en |
| dc.language.iso | fr | fr_FR |
| dc.publisher | Masson, Paris | fr_FR |
| dc.rights | Article en libre accès | fr |
| dc.rights | Médecine/Sciences - Inserm - SRMS | fr |
| dc.source | M/S. Médecine sciences [revue papier, ISSN : 0767-0974], 1999, Vol. 15, N° 3; p.359-68 | fr_FR |
| dc.title | Mécanismes ioniques des altérations de la repolarisation cardiaque dans les cardiopathies. | fr |
| dc.title.alternative | Ionic mechanisms and repolarization alterations in cardiopathies | fr_FR |
| dc.type | Article | fr_FR |
| dc.contributor.affiliation | Cnrs SA 8078, Laboratoire de cardiologie moleculaire et cellulaire, Hopital Marie-Lannelongue, 92350 Le Plessis-Robinson, France | - |
| dc.identifier.doi | 10.4267/10608/1346 | |