| dc.contributor.author | Lacaze-Masmonteil, T | fr_FR |
| dc.contributor.author | Thébaud, B | fr_FR |
| dc.date.accessioned | 2012-08-23T13:57:01Z | |
| dc.date.available | 2012-08-23T13:57:01Z | |
| dc.date.issued | 1999 | fr_FR |
| dc.identifier.citation | Lacaze-Masmonteil, T - Thébaud, B, Avancées thérapeutiques dans la prise en charge des détresses respiratoires du nouveau-né., Med Sci (Paris), 1999, Vol. 15, N° 6-7; p.788-97 | fr_FR |
| dc.identifier.issn | 1958-5381 | fr_FR |
| dc.identifier.uri | http://hdl.handle.net/10608/1435 | |
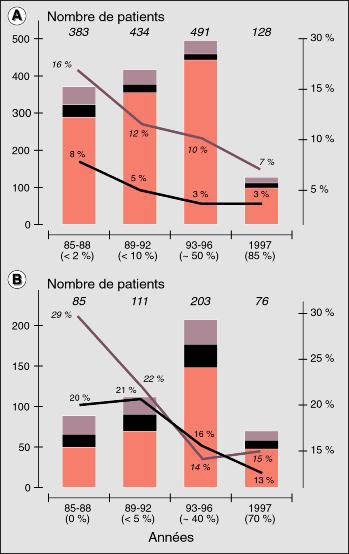
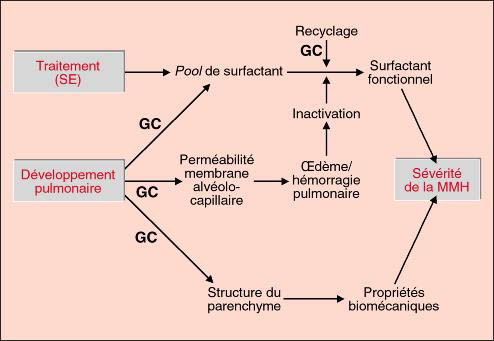
| dc.description.abstract | Les progres de la reanimation respiratoire en neonatalogie rendent compte de la diminution importante et reguliere de la mortalite perinatale des enfants prematures observee ces 15 dernieres annees. Deux traitements complementaires ont fait leur preuve. La corticotherapie antenatale accelere la maturation pulmonaire et reduit la frequence de survenue du syndrome de detresse respiratoire. L' utilisation des surfactants exogenes, immediatement apres la naissance, diminue la frequence des complications barotraumatiques et augmente le taux de survivants sans sequelle respiratoire. Chez le nouveau-ne a terme, la necessite d' un recours aux methodes d' oxygenation extracorporelle a considerablement diminue grace au developpement de la ventilation a haute frequence et a l' introduction du monoxyde d' azote inhale. Le benefice de ces deux dernieres strategies chez le premature est encore en cours d' evaluation. | fr |
| dc.description.abstract | Prevention and treatment of neonatal respiratory distress syndrome have dramatically improved over the past fifteen years, leading to a striking reduction in perinatal mortality among very premature infants. Data from numerous experimental studies clearly indicate that both endogenous and exogenous corticosteroids accelerate fetal lung maturation. Several controlled trial and meta-analyses have confirmed the efficiency of antenatal glucocorticoids administration in reducing neonatal mortality, the prevalence of respiratory distress syndrome, and the odds of several severe complications relating to immaturity. Exogenous surfactant therapy does not rule out the benefits of corticosteroids. On the contrary, there is synergism between antenatal hormone treatment and postnatal surfactant administration. Improvements in neonatal morbidity and mortality have been demonstrated for premature infants treated with various exogenous surfactant preparations. Inactivation of surfactant is often involved in the pathogenesis of several respiratory disorders of the full-term or near full term baby: recent clinical reports suggest that early administration of exogenous surfactant in severe meconial aspiration may be beneficial, by reducing extracorporeal membrane oxygenation utilization. Whether synthetic surfactants containing phospholipids and chemically or genetically engineered homologous peptides may be as beneficial as natural surfactant is presently addressed by several ongoing trials. Inhaled nitric oxide improves gas exchanges and decreases pulmonary vascular resistance in newborn with persistent pulmonary hypertension. Several multicenter trials have demonstrated that inhaled nitric oxide reduces the need for extracorporeal membrane oxygenation in full term or near full term neonates with severe hypoxemia. Preliminary results suggest that inhaled nitric oxide may be also beneficial in preterm infants. There is a consensus that high frequency ventilation may be useful for the rescue therapy of newborns with respiratory failure which does not respond to conventional ventilation. In contrast, whether high frequency ventilation should replace conventional ventilation in the early management of respiratory distress syndrome remains under question. Preliminary pilot studies have shown that partial liquid ventilation can be used in preterm patients; however, the benefit of this therapy compared to an optimal conventional approach is questionable. A less agressive management combining antenatal steroids exposure, early nasal cPAP and surfactant administration following a short intubation appears promising for the prevention of chronic lung disease; the benefit of this "mini-touch" approach remains to be demonstrated by prospective trials. | en |
| dc.language.iso | fr | fr_FR |
| dc.publisher | Masson Périodiques, Paris | fr_FR |
| dc.rights | Article en libre accès | fr |
| dc.rights | Médecine/Sciences - Inserm - SRMS | fr |
| dc.source | M/S. Médecine sciences [revue papier, ISSN : 0767-0974], 1999, Vol. 15, N° 6-7; p.788-97 | fr_FR |
| dc.title | Avancées thérapeutiques dans la prise en charge des détresses respiratoires du nouveau-né. | fr |
| dc.title.alternative | New strategies for respiratory failure in newborns | fr_FR |
| dc.type | Article | fr_FR |
| dc.contributor.affiliation | Service de Pediatrie et Reanimation Neonatales, Hopital Antoine-Beclere (AP-HP), 157, rue de la porte de Trivaux, 92140 Clamart, France | - |
| dc.identifier.doi | 10.4267/10608/1435 | |