| dc.contributor.author | Duclos-Vallée, Jean-Charles | - |
| dc.contributor.author | Teicher, Elina | - |
| dc.contributor.author | Vittecoq, Daniel | - |
| dc.contributor.author | Samuel, Didier | - |
| dc.date.accessioned | 2014-08-13T07:16:25Z | |
| dc.date.available | 2014-08-13T07:16:25Z | |
| dc.date.issued | 2007 | fr_FR |
| dc.identifier.citation | Duclos-Vallée, Jean-Charles ; Teicher, Elina ; Vittecoq, Daniel ; Samuel, Didier ; La transplantation hépatique chez les patients co-infectés VIH/VHC et VIH/VHB, Med Sci (Paris), 2007, Vol. 23, N° 8-9; p. 723-728 ; DOI : 10.1051/medsci/20072389723 | fr_FR |
| dc.identifier.issn | 1958-5381 | fr_FR |
| dc.identifier.uri | http://hdl.handle.net/10608/6230 | |
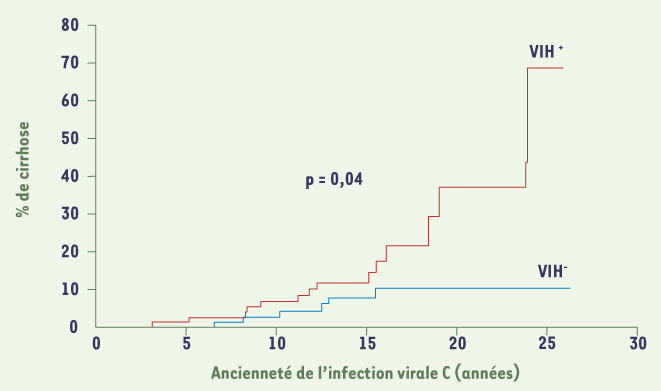
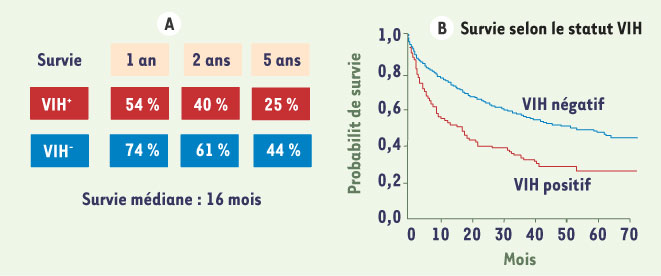
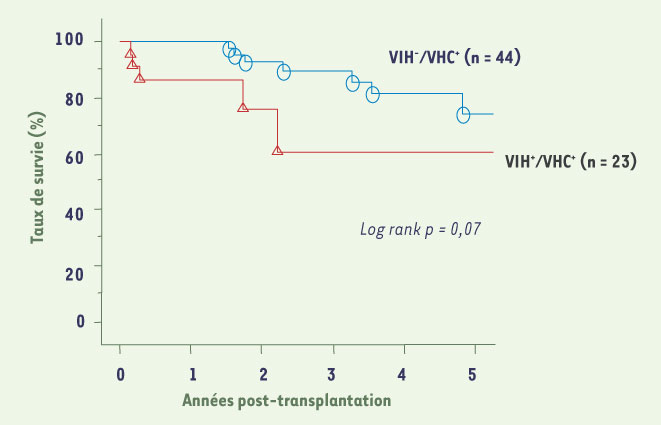
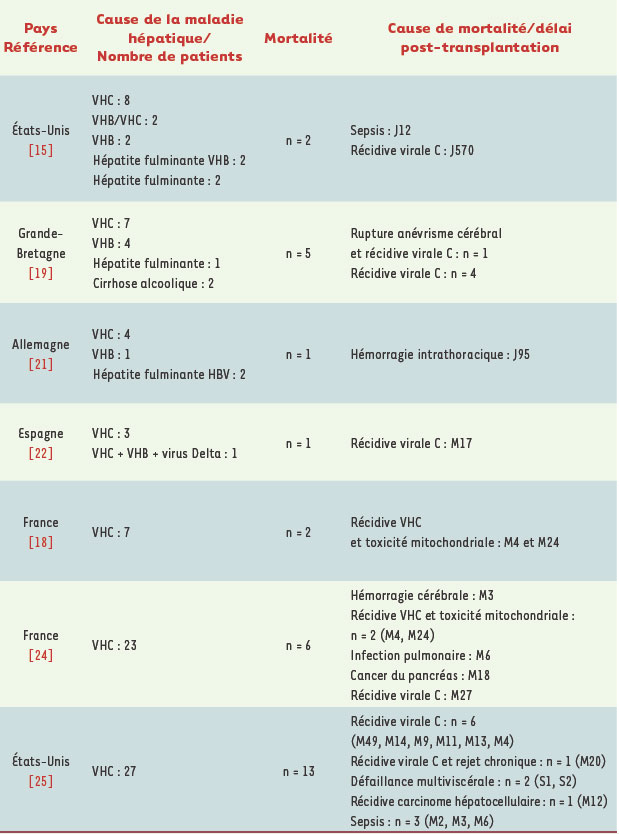
| dc.description.abstract | L’infection par le virus de l’immunodéficience humaine (VIH) a longtemps été considérée comme une contre-indication à la transplantation hépatique. Les raisons en étaient le pronostic sombre lié à la maladie VIH. L’avènement des trithérapies antirétrovirales a révolutionné le traitement des patients infectés par le VIH. Trente pour cent et 10 % des patients infectés par le VIH sont également infectés respectivement par le virus de l’hépatite C (VHC) et par le virus de l’hépatite B (VHB). L’hépatite chronique C et B semble progresser plus vite chez les patients co-infectés et un nombre important de patients développent une cirrhose menaçant le pronostic vital. La transplantation hépatique pose plusieurs problèmes dans ce contexte : (1) le risque d’accident d’exposition au sang lors de cette intervention longue et hémorragique ; (2) le moment de l’indication de la transplantation ; (3) l’interférence entre les antirétroviraux et les inhibiteurs de la calcineurine ; (4) le risque de récidive du VHB ou du VHC. Depuis 1999, un programme de transplantation hépatique chez les patients co-infectés a démarré avec le soutien de l’Agence nationale de recherche contre le sida et les hépatites. Les premiers résultats montrent une survie à 2 ans de 70 % des patients infectés par le VHC et de 100 % des patients infectés par le VHB. Il n’a pas été noté de progression accélérée de la maladie VIH. La récidive virale B est bien prévenue par l’association post-transplantation d’immunoglobulines spécifiques anti-HBs et d’analogues nucléosidiques et nucléotidiques efficaces contre le VHB. La difficulté majeure est la récidive virale C. L’identification de ses mécanismes, sa prévention et son traitement sont les futurs défis à résoudre. | fr |
| dc.description.abstract | Human immunodeficiency virus infection (HIV) has been considered until recently as a contraindication for liver transplantation. This was due to the poor spontaneous prognosis of HIV infection. The advent of highly active antiretroviral drugs (HAART) was a therapeutic breakthrough, and the prognosis has been dramatically improved. 30 % and 10 % of HIV infected patients are coinfected with hepatitis C virus (HCV) and with hepatitis B virus (HBV), respectively. The progression of chronic hepatitis B and C seems more rapid in coinfected patients, and a high number of patients will develop life-threatening liver cirrhosis. There are numerous potential problems raised by liver transplantation in HIV infected patients: (1) the potential risk of needlestick injury during this type of hemorrhagic surgery at high risk of bleeding ; (2) the timing for liver transplantation ; (3) the risk of interference between HAART and calcineurin inhibitors ; (4) The risk of HBV and HCV recurrence post-transplant. Since 1999, a program of liver transplantation has been started in patients coinfected with HIV and HBV or HCV with the support of the Agence Nationale de Recherche contre le Sida et les Hépatites virales (ANRS). The first results showed that liver transplantation in HIV-HCV and HIV-HBV infected patients is feasible, achieving 2-year survival of 70 % and 100 %, respectively. There was no acceleration of HIV disease after transplantation. HBV recurrence was well prevented by the combination of anti-HBs immunoglobulins plus nucleoside and nucleotide analogues effective against HBV. The main problem is HCV recurrence, which is more rapid and more severe in HIV coinfected patients than in HCV monoinfected patients. Understanding HCV recurrence mechanisms, and preventing and treating of HCV recurrence are major future challenges. | en |
| dc.language.iso | fr | fr_FR |
| dc.publisher | EDK | fr_FR |
| dc.relation.ispartof | M/S revues | fr_FR |
| dc.rights | Article en libre accès | fr |
| dc.rights | Médecine/Sciences - Inserm - SRMS | fr |
| dc.source | M/S. Médecine sciences [ISSN papier : 0767-0974 ; ISSN numérique : 1958-5381], 2007, Vol. 23, N° 8-9; p. 723-728 | fr_FR |
| dc.subject.mesh | Cause de décès | fr |
| dc.subject.mesh | Infections à VIH | fr |
| dc.subject.mesh | Hépatite B | fr |
| dc.subject.mesh | Hépatite C | fr |
| dc.subject.mesh | Humains | fr |
| dc.subject.mesh | Transplantation hépatique | fr |
| dc.subject.mesh | Sélection de patients | fr |
| dc.subject.mesh | Analyse de survie | fr |
| dc.subject.mesh | Survivants | fr |
| dc.title | La transplantation hépatique chez les patients co-infectés VIH/VHC et VIH/VHB | fr |
| dc.title.alternative | Liver transplantation for patients infected with both HIV and HCV or HIV and HBV | en |
| dc.type | Article | fr_FR |
| dc.contributor.affiliation | Département des Maladies du Foie et Inserm U 785 | fr_FR |
| dc.contributor.affiliation | Unité de Maladies infectieuses. Université Paris XI, Centre Hépato-Biliaire, Hôpital Paul Brousse,12-14, avenue Paul Vaillant Couturier, 94804 Villejuif, France | fr_FR |
| dc.identifier.doi | 10.1051/medsci/20072389723 | fr_FR |
| dc.identifier.pmid | 17875290 | fr_FR |